Wednesday, September 30, 2009
The Cost of Care, Part 2
The second part of the Dallas Morning News’ five part series called “The Cost of Care” tackled the doctor-owned hospital dilemma. You can access the series here. The article does a fantastic job of examining physician-owned hospitals from a variety of angles, admitting that it is a complex issue and that not all physician-owned facilities are created equal. We know that some physician/system
The Cost of Care, Part 2
The second part of the Dallas Morning News’ five part series called “The Cost of Care” tackled the doctor-owned hospital dilemma. You can access the series here. The article does a fantastic job of examining physician-owned hospitals from a variety of angles, admitting that it is a complex issue and that not all physician-owned facilities are created equal. We know that some physician/system
Green Tea And Stomach Cancer
Researchers have studied green tea in cancer prevention because they suspect that the drink's antioxidants may protect against the disease. In particular, it may include compounds that fight bacteria that have been linked to stomach cancer. A new study by Dr. M. Inoue, at the National Cancer Center in Tokyo, examined six older studies.
Together, these studies involved more than 219,000 men and women 40 years and older, who were followed from about 7 years to more than 11 years. Overall, about four in five of the participants reported drinking green tea daily, with about a third drinking five or more cups per day.
During follow-up, about 2500 of the approximately 100,000 men, and about 1000 of the more than 118,000 women in the studies developed stomach cancer.
The researchers found no link between more tea drinking and reduced stomach cancer risk among men.
The 20 percent reduced stomach cancer risk they saw among women drinking 5 or more, versus 1 or less, cups of green tea daily remained true even after the researchers took smoking into account.
Read more about this study >>
Don't fancy drinking green tea? then take a green tea supplement instead.
Together, these studies involved more than 219,000 men and women 40 years and older, who were followed from about 7 years to more than 11 years. Overall, about four in five of the participants reported drinking green tea daily, with about a third drinking five or more cups per day.
During follow-up, about 2500 of the approximately 100,000 men, and about 1000 of the more than 118,000 women in the studies developed stomach cancer.
The researchers found no link between more tea drinking and reduced stomach cancer risk among men.
The 20 percent reduced stomach cancer risk they saw among women drinking 5 or more, versus 1 or less, cups of green tea daily remained true even after the researchers took smoking into account.
Read more about this study >>
Don't fancy drinking green tea? then take a green tea supplement instead.
Memo to White House Speechwriters
Feel free to insert this into President Obama's next speech:
"There has been a lot of talk lately about taxing Cadillac health plans. Well, I have thought about this idea, and I have talked with my economic advisers, and we have decided that it indeed makes a lot of sense.
"Now some of you may wonder whether endorsing this proposal breaks my pledge not to raise taxes on the middle class. After all, you don't need to be rich to drive a Cadillac, and you don't need to be rich to have a Cadillac health plan. So, hereafter, I will refer to them as Rolls Royce health plans.
"Seriously, though: Yes, it is a tax increase on the middle class. When I said during the campaign that I would raise taxes only on the rich, I meant it. Or at least I wanted to mean it. But my damn economic advisers keep bugging me about the laws of arithmetic. And, you know, they are right. I am more interested in expanding entitlements than reining them in, so I don't have much choice but to raise taxes on the vast majority of Americans. If you think this Cadillac tax is the end of it, you just wait.
"I also know that this tax offends some of my supporters in the union movement, who now enjoy the benefits of Cadillac health plans. But how much do you guys expect from me? I have already thrown you the bone of a completely unjustifiable tariff on Chinese tires, risking a trade war in the midst of a global economic downturn. You guys should be happy with that. Will you please get off my case?
"Finally, I need to make an apology. No, not to Europe for Bush-era foreign policy this time. But to Senator McCain. During the campaign, I lambasted you for proposing to tax health insurance benefits. I knew at the time that your goals were laudable--to finance tax credits for lower income families and to rein in tax incentives for excessive insurance. And indeed your proposal was not very different from the tax on Cadillac plans that is now being considered in Congress and that I will gladly sign into law. But the issue offered just too good of a sound bite to give up. Now that I am safely in the White House, however, I am man enough to admit that Senator McCain was right all along, and I was wrong. Gosh, it feels good to get that off my chest."
"There has been a lot of talk lately about taxing Cadillac health plans. Well, I have thought about this idea, and I have talked with my economic advisers, and we have decided that it indeed makes a lot of sense.
"Now some of you may wonder whether endorsing this proposal breaks my pledge not to raise taxes on the middle class. After all, you don't need to be rich to drive a Cadillac, and you don't need to be rich to have a Cadillac health plan. So, hereafter, I will refer to them as Rolls Royce health plans.
"Seriously, though: Yes, it is a tax increase on the middle class. When I said during the campaign that I would raise taxes only on the rich, I meant it. Or at least I wanted to mean it. But my damn economic advisers keep bugging me about the laws of arithmetic. And, you know, they are right. I am more interested in expanding entitlements than reining them in, so I don't have much choice but to raise taxes on the vast majority of Americans. If you think this Cadillac tax is the end of it, you just wait.
"I also know that this tax offends some of my supporters in the union movement, who now enjoy the benefits of Cadillac health plans. But how much do you guys expect from me? I have already thrown you the bone of a completely unjustifiable tariff on Chinese tires, risking a trade war in the midst of a global economic downturn. You guys should be happy with that. Will you please get off my case?
"Finally, I need to make an apology. No, not to Europe for Bush-era foreign policy this time. But to Senator McCain. During the campaign, I lambasted you for proposing to tax health insurance benefits. I knew at the time that your goals were laudable--to finance tax credits for lower income families and to rein in tax incentives for excessive insurance. And indeed your proposal was not very different from the tax on Cadillac plans that is now being considered in Congress and that I will gladly sign into law. But the issue offered just too good of a sound bite to give up. Now that I am safely in the White House, however, I am man enough to admit that Senator McCain was right all along, and I was wrong. Gosh, it feels good to get that off my chest."
CT Health Policy Project turns ten
The number of CT residents living without health insurance is up 18% in the last ten years. Ten years ago the CT Health Policy Project began our work to improve access to quality, affordable health care for every CT resident. In the last ten years we’ve published 223 analyses, briefs and studies and mentored 43 students. To mark the occasion we asked nine prominent CT stakeholders to reflect on how health care has changed in our state in the last decade and make predictions for the future. Contributors include Pat Baker of the CT Health Foundation, Congressman Joe Courtney, former Congresswoman Nancy Johnson, Sen. Edith Prague, Rep. Betsy Ritter, Gary Spinner PA, Hillary Waldman of the Hispanic Health Council and former Hartford Courant health reporter, State Comptroller Nancy Wyman and Jill Zorn of the Universal Health Care Foundation of CT.
The CT Health Policy Project wants to thank the many students, volunteers, interns, fellows, Board members, funders, collaborators, donors, staff, clients, bureaucrats, elected officials, very supportive family and friends who have made the last ten years not only possible, but a joy. We all get five minutes to reflect, then back to work.
Ellen Andrews
The CT Health Policy Project wants to thank the many students, volunteers, interns, fellows, Board members, funders, collaborators, donors, staff, clients, bureaucrats, elected officials, very supportive family and friends who have made the last ten years not only possible, but a joy. We all get five minutes to reflect, then back to work.
Ellen Andrews
Tuesday, September 29, 2009
Malocclusion: Disease of Civilization
In his epic work Nutrition and Physical Degeneration, Dr. Weston Price documented the abnormal dental development and susceptibility to tooth decay that accompanied the adoption of modern foods in a number of different cultures throughout the world. Although he quantified changes in cavity prevalence (sometimes finding increases as large as 1,000-fold), all we have are Price's anecdotes describing the crooked teeth, narrow arches and "dished" faces these cultures developed as they modernized.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph: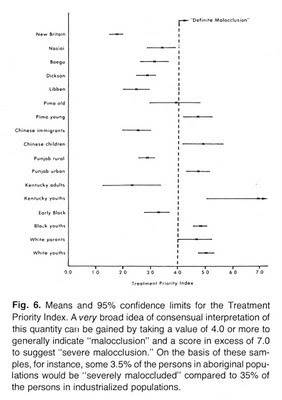 Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.
Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.
The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
- Class I occlusion: considered "ideal". The bottom incisors (front teeth) fit just behind the top incisors.
- Class II occlusion: "overbite." The bottom incisors are too far behind the top incisors. The mandible may appear small.
- Class III occlusion: "underbite." The bottom incisors are beyond the top incisors. The mandible protrudes.
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:
 Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.
Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
I assert that these results serve to modify two widespread generalizations: that imperfect occlusion is not necessarily abnormal, and that prevalence of malocclusion is genetically controlled so that preventive therapy in the strict sense is not possible. Cross-cultural data dispel the notion that considerable occlusal variation [malocclusion] is inevitable or normal. Rather, it is an aberrancy of modern urbanized populations. Furthermore, the transition from predominantly good to predominantly bad occlusion repeatedly occurs within one or two generations' time in these (and other) populations, weakening arguments that explain high malocclusion prevalence genetically.
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Malocclusion: Disease of Civilization
In his epic work Nutrition and Physical Degeneration, Dr. Weston Price documented the abnormal dental development and susceptibility to tooth decay that accompanied the adoption of modern foods in a number of different cultures throughout the world. Although he quantified changes in cavity prevalence (sometimes finding increases as large as 1,000-fold), all we have are Price's anecdotes describing the crooked teeth, narrow arches and "dished" faces these cultures developed as they modernized.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.
The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
- Class I occlusion: considered "ideal". The bottom incisors (front teeth) fit just behind the top incisors.
- Class II occlusion: "overbite." The bottom incisors are too far behind the top incisors. The mandible may appear small.
- Class III occlusion: "underbite." The bottom incisors are beyond the top incisors. The mandible protrudes.
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:
Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
I assert that these results serve to modify two widespread generalizations: that imperfect occlusion is not necessarily abnormal, and that prevalence of malocclusion is genetically controlled so that preventive therapy in the strict sense is not possible. Cross-cultural data dispel the notion that considerable occlusal variation [malocclusion] is inevitable or normal. Rather, it is an aberrancy of modern urbanized populations. Furthermore, the transition from predominantly good to predominantly bad occlusion repeatedly occurs within one or two generations' time in these (and other) populations, weakening arguments that explain high malocclusion prevalence genetically.
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Malocclusion: Disease of Civilization
In his epic work Nutrition and Physical Degeneration, Dr. Weston Price documented the abnormal dental development and susceptibility to tooth decay that accompanied the adoption of modern foods in a number of different cultures throughout the world. Although he quantified changes in cavity prevalence (sometimes finding increases as large as 1,000-fold), all we have are Price's anecdotes describing the crooked teeth, narrow arches and "dished" faces these cultures developed as they modernized.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.
The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
- Class I occlusion: considered "ideal". The bottom incisors (front teeth) fit just behind the top incisors.
- Class II occlusion: "overbite." The bottom incisors are too far behind the top incisors. The mandible may appear small.
- Class III occlusion: "underbite." The bottom incisors are beyond the top incisors. The mandible protrudes.
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:
Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
I assert that these results serve to modify two widespread generalizations: that imperfect occlusion is not necessarily abnormal, and that prevalence of malocclusion is genetically controlled so that preventive therapy in the strict sense is not possible. Cross-cultural data dispel the notion that considerable occlusal variation [malocclusion] is inevitable or normal. Rather, it is an aberrancy of modern urbanized populations. Furthermore, the transition from predominantly good to predominantly bad occlusion repeatedly occurs within one or two generations' time in these (and other) populations, weakening arguments that explain high malocclusion prevalence genetically.
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Malocclusion: Disease of Civilization
In his epic work Nutrition and Physical Degeneration, Dr. Weston Price documented the abnormal dental development and susceptibility to tooth decay that accompanied the adoption of modern foods in a number of different cultures throughout the world. Although he quantified changes in cavity prevalence (sometimes finding increases as large as 1,000-fold), all we have are Price's anecdotes describing the crooked teeth, narrow arches and "dished" faces these cultures developed as they modernized.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.
The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Price published the first edition of his book in 1939. Fortunately, Nutrition and Physical Degeneration wasn't the last word on the matter. Anthropologists and archaeologists have been extending Price's findings throughout the 20th century. My favorite is Dr. Robert S. Corruccini, currently a professor of anthropology at Southern Illinois University. He published a landmark paper in 1984 titled "An Epidemiologic Transition in Dental Occlusion in World Populations" that will be our starting point for a discussion of how diet and lifestyle factors affect the development of the teeth, skull and jaw (Am J. Orthod. 86(5):419)*.
First, some background. The word occlusion refers to the manner in which the top and bottom sets of teeth come together, determined in part by the alignment between the upper jaw (maxilla) and lower jaw (mandible). There are three general categories:
- Class I occlusion: considered "ideal". The bottom incisors (front teeth) fit just behind the top incisors.
- Class II occlusion: "overbite." The bottom incisors are too far behind the top incisors. The mandible may appear small.
- Class III occlusion: "underbite." The bottom incisors are beyond the top incisors. The mandible protrudes.
Over the course of the next several posts, I'll give an overview of the extensive literature showing that hunter-gatherers past and present have excellent occlusion, subsistence agriculturalists generally have good occlusion, and the adoption of modern foodways directly causes the crooked teeth, narrow arches and/or crowded third molars (wisdom teeth) that affect the majority of people in industrialized nations. I believe this process also affects the development of the rest of the skull, including the face and sinuses.
In his 1984 paper, Dr. Corruccini reviewed data from a number of cultures whose occlusion has been studied in detail. Most of these cultures were observed by Dr. Corruccini personally. He compared two sets of cultures: those that adhere to a traditional style of life and those that have adopted industrial foodways. For several of the cultures he studied, he compared it to another that was genetically similar. For example, the older generation of Pima indians vs. the younger generation, and rural vs. urban Punjabis. He also included data from archaeological sites and nonhuman primates. Wild animals, including nonhuman primates, almost invariably show perfect occlusion.
The last graph in the paper is the most telling. He compiled all the occlusion data into a single number called the "treatment priority index" (TPI). This is a number that represents the overall need for orthodontic treatment. A TPI of 4 or greater indicates malocclusion (the cutoff point is subjective and depends somewhat on aesthetic considerations). Here's the graph:
Every single urban/industrial culture has an average TPI of greater than 4, while all the non-industrial or less industrial cultures have an average TPI below 4. This means that in industrial cultures, the average person requires orthodontic treatment to achieve good occlusion, whereas most people in more traditionally-living cultures naturally have good occlusion.The best occlusion was in the New Britain sample, a precontact Melanesian hunter-gatherer group studied from archaeological remains. The next best occlusion was in the Libben and Dickson groups, who were early Native American agriculturalists. The Pima represent the older generation of Native Americans that was raised on a somewhat traditional agricultural diet, vs. the younger generation raised on processed reservation foods. The Chinese samples are immigrants and their descendants in Liverpool. The Punjabis represent urban vs. rural youths in Northern India. The Kentucky samples represent a traditionally-living Appalachian community, older generation vs. processed food-eating offspring. The "early black" and "black youths" samples represent older and younger generations of African-Americans in the Cleveland and St. Louis area. The "white parents/youths" sample represents different generations of American Caucasians.
The point is clear: there's something about industrialization that causes malocclusion. It's not genetic; it's a result of changes in diet and/or lifestyle. A "disease of civilization". I use that phrase loosely, because malocclusion isn't really a disease, and some cultures that qualify as civilizations retain traditional foodways and relatively good teeth. Nevertheless, it's a time-honored phrase that encompasses the wide array of health problems that occur when humans stray too far from their ecological niche. I'm going to let Dr. Corruccini wrap this post up for me:
I assert that these results serve to modify two widespread generalizations: that imperfect occlusion is not necessarily abnormal, and that prevalence of malocclusion is genetically controlled so that preventive therapy in the strict sense is not possible. Cross-cultural data dispel the notion that considerable occlusal variation [malocclusion] is inevitable or normal. Rather, it is an aberrancy of modern urbanized populations. Furthermore, the transition from predominantly good to predominantly bad occlusion repeatedly occurs within one or two generations' time in these (and other) populations, weakening arguments that explain high malocclusion prevalence genetically.
* This paper is worth reading if you get the chance. It should have been a seminal paper in the field of preventive orthodontics, which could have largely replaced conventional orthodontics by now. Dr. Corruccini is the clearest thinker on this subject I've encountered so far.
Hepatitis C Strike Public EmployeesMan
Surveys by the Department of Health of Indonesia said that more private sector employees disease hepatitis C rather than civil servants. The disease is fatal liver infection and symptoms are not even that much more experienced men than women.
This was stated by Dr. Andi Muhaidin, Sepimkesma Director of Disease Control and Environmental Health (PP & PL) in the Seminar Problems in Indonesia Hepatitis C held at the Hotel Gran Melia, Jakarta, Tuesday (29/9/2009). On that occasion also conducted the handover data collection program of the National Hepatitis C PT Roche Indonesia to the Ministry of Health Indonesia.
"I do not know why it happened, but the results of our survey in the field based on professional categories show like that," said Andi. Responding to data released by the Ministry of Health, Chief Researcher Heart Association Indonesia (PPHI), Dr. Superior Budihusodo, SpPD-KGEH can not yet fully explain these facts.
"That's discoveries in the field, I also do not know why because there are no studies that explain it. But private sector employees who are infected also depends on profession. Professions such as doctors, nurses, medical workers and those who are often associated with blood transfusion are most at risk of infection viral hepatitis C. They are all his most private sector employees, so a higher prevalence than public servants, "explained Superior.
Number of private sector employees more than any civil servant may be able to explain the facts in the field. "But definitely, the prevalence of hepatitis C was high into the population we are at risk," said Superior.
Other risks that should be aware of the male group. According to MOH data, the risk of hepatitis C in men was 83 percent, while women only about 17 percent.
"Up until now could not explain why, but probably because men are relatively more 'active' or 'pocket' anywhere. But it is clear that the risk of contracting the higher man. She was lucky to get a little but a lot is better. If a man , many of which hit hard but its recovery. So that was lucky woman, "said Superior.
Hepatitis C is one type of viral infection of the liver resulting in inflammation and liver damage if it is severe and can lead to liver damage, cirrhosis (hardening) the liver, liver cancer and death.
Usually the disease around age 20 to 30 years. But because this disease does not address the physical symptoms, so most people do not realize he hit Hepatitis C. Suddenly, after the doctor had checked into a chronic condition, acute and even cirrhosis. If it's so life expectancy is usually less than 1 year.
According to the World Health Organization (WHO), approximately 170 million people infected with hepatitis C virus (VHC). Compared to European countries, Africa and America, countries in Southeast Asia are infected more is about 32.3 percent of the total world population.
In Indonesia alone there are an estimated 7 million people who suffer from this virus, but until now there has been no vaccine that can prevent virus transmission because of the nature mutate very easily.
This was stated by Dr. Andi Muhaidin, Sepimkesma Director of Disease Control and Environmental Health (PP & PL) in the Seminar Problems in Indonesia Hepatitis C held at the Hotel Gran Melia, Jakarta, Tuesday (29/9/2009). On that occasion also conducted the handover data collection program of the National Hepatitis C PT Roche Indonesia to the Ministry of Health Indonesia.
"I do not know why it happened, but the results of our survey in the field based on professional categories show like that," said Andi. Responding to data released by the Ministry of Health, Chief Researcher Heart Association Indonesia (PPHI), Dr. Superior Budihusodo, SpPD-KGEH can not yet fully explain these facts.
"That's discoveries in the field, I also do not know why because there are no studies that explain it. But private sector employees who are infected also depends on profession. Professions such as doctors, nurses, medical workers and those who are often associated with blood transfusion are most at risk of infection viral hepatitis C. They are all his most private sector employees, so a higher prevalence than public servants, "explained Superior.
Number of private sector employees more than any civil servant may be able to explain the facts in the field. "But definitely, the prevalence of hepatitis C was high into the population we are at risk," said Superior.
Other risks that should be aware of the male group. According to MOH data, the risk of hepatitis C in men was 83 percent, while women only about 17 percent.
"Up until now could not explain why, but probably because men are relatively more 'active' or 'pocket' anywhere. But it is clear that the risk of contracting the higher man. She was lucky to get a little but a lot is better. If a man , many of which hit hard but its recovery. So that was lucky woman, "said Superior.
Hepatitis C is one type of viral infection of the liver resulting in inflammation and liver damage if it is severe and can lead to liver damage, cirrhosis (hardening) the liver, liver cancer and death.
Usually the disease around age 20 to 30 years. But because this disease does not address the physical symptoms, so most people do not realize he hit Hepatitis C. Suddenly, after the doctor had checked into a chronic condition, acute and even cirrhosis. If it's so life expectancy is usually less than 1 year.
According to the World Health Organization (WHO), approximately 170 million people infected with hepatitis C virus (VHC). Compared to European countries, Africa and America, countries in Southeast Asia are infected more is about 32.3 percent of the total world population.
In Indonesia alone there are an estimated 7 million people who suffer from this virus, but until now there has been no vaccine that can prevent virus transmission because of the nature mutate very easily.
src="http://pagead2.googlesyndication.com/pagead/show_ads.js" type="text/javascript">
Oats Coconut Milk Pudding(Pradhaman)...No Eggs Needed.

Pradhaman in all its creamy and coconutty flavors reflects the exotic coastal state of Kerala in South India.The pudding makes the sweet side of the Sadya(big feast) served on banana leaf.Usually made with rice flakes,the whole oats seem to work just fine as the substitute for it.This delectable dessert is the creation of Madhuram at Eggless cooking,the blog with amazing eggless baking ideas,is also featured this month for Tried and Tasted event,the hostess of the month is Poornima of Tasty treats.
Recipe adapted from Madhuram's Eggless Cooking

Ingredients
1/2 cup Whole rolled oats
*1/4 cup Jaggery ,grated[available in most Asian stores)
1 cup Water
1 cup(about 4 ounce) Lite Coconut Milk
Roasted nuts and dried fruits for garnish
*If Jaggery is hard to find use 2 tablespoon brown or white sugar,or 3 teaspoon Agave nectar.
Method
In a heavy bottom sauce pan add the jaggery ,oats and water.Bring to a slow boil and cook until oats are softened.Reduce the heat and add the coconut milk,let simmer for 4-5 minutes until thick and creamy.Serve warm ,garnish with roasted nuts and dried fruits.
Food Facts
Jaggery - Healthier Substitute for Refined Sugar

Jaggery is common in South Asian desserts and Candies.Produced by boiling raw sugar cane or palm juice,jaggery does not under go additional processing hence is richer in natural nutrients.Jaggery also has several health benefits according to the traditional Indian medicine of Ayurveda including respiratory illness and maintaining blood pressure.
Teachers lead with germiest work environments
As cold and flu season approaches, the WSJ blog has identified the occupations most likely to encounter germs. As expected, teachers lead the list with twenty times the germs per square inch of attorneys who have the cleanest offices. Teachers’ phones are the main culprit, accountants have the dirtiest desks and you don’t want to touch a banker’s computer mouse or door knob. Women’s offices are dirtier than men’s but are less likely to have MRSA.
Ellen Andrews
Ellen Andrews
Monday, September 28, 2009
Diabetics on a Low-carbohydrate Diet, Part II
I just found another very interesting study performed in Japan by Dr. Hajime Haimoto and colleagues (free full text). They took severe diabetics with an HbA1c of 10.9% and put them on a low-carbohydrate diet:
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
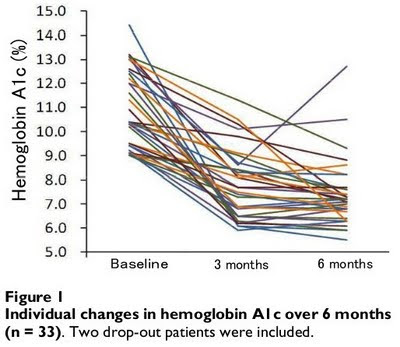 Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
The main principle of the CRD [carbohydrate-restricted diet] was to eliminate carbohydrate-rich food twice a day at breakfast and dinner, or eliminate it three times a day at breakfast, lunch and dinner... There were no other restrictions. Patients on the CRD were permitted to eat as much protein and fat as they wanted, including saturated fat.What happened to their blood lipids after eating all that fat for 6 months, and increasing their saturated fat intake to that of the average American? LDL decreased and HDL increased, both statistically significant. Oops. But that's water under the bridge. What we really care about here is glucose control. The patients' HbA1c (glycated hemoglobin; a measure of average blood glucose over the past several weeks) declined from 10.9 to 7.4%.
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
 Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:One female patient had an increased physical activity level during the study period in spite of our instructions. However, her increase in physical activity was no more than one hour of walking per day, four days a week. She had implemented an 11% carbohydrate diet without any antidiabetic drug, and her HbA1c level decreased from 14.4% at baseline to 6.1% after 3 months and had been maintained at 5.5% after 6 months.That patient began with the highest HbA1c and ended with the lowest. Complete glucose control using only diet and exercise. It may not work for everyone, but it's effective in some cases. The study's conclusion:
...the 30%-carbohydrate diet over 6 months led to a remarkable reduction in HbA1c levels, even among outpatients with severe type 2 diabetes, without any insulin therapy, hospital care or increase in sulfonylureas. The effectiveness of the diet may be comparable to that of insulin therapy.
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
Diabetics on a Low-carbohydrate Diet, Part II
I just found another very interesting study performed in Japan by Dr. Hajime Haimoto and colleagues (free full text). They took severe diabetics with an HbA1c of 10.9% and put them on a low-carbohydrate diet:
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
The main principle of the CRD [carbohydrate-restricted diet] was to eliminate carbohydrate-rich food twice a day at breakfast and dinner, or eliminate it three times a day at breakfast, lunch and dinner... There were no other restrictions. Patients on the CRD were permitted to eat as much protein and fat as they wanted, including saturated fat.What happened to their blood lipids after eating all that fat for 6 months, and increasing their saturated fat intake to that of the average American? LDL decreased and HDL increased, both statistically significant. Oops. But that's water under the bridge. What we really care about here is glucose control. The patients' HbA1c (glycated hemoglobin; a measure of average blood glucose over the past several weeks) declined from 10.9 to 7.4%.
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:One female patient had an increased physical activity level during the study period in spite of our instructions. However, her increase in physical activity was no more than one hour of walking per day, four days a week. She had implemented an 11% carbohydrate diet without any antidiabetic drug, and her HbA1c level decreased from 14.4% at baseline to 6.1% after 3 months and had been maintained at 5.5% after 6 months.That patient began with the highest HbA1c and ended with the lowest. Complete glucose control using only diet and exercise. It may not work for everyone, but it's effective in some cases. The study's conclusion:
...the 30%-carbohydrate diet over 6 months led to a remarkable reduction in HbA1c levels, even among outpatients with severe type 2 diabetes, without any insulin therapy, hospital care or increase in sulfonylureas. The effectiveness of the diet may be comparable to that of insulin therapy.
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
Diabetics on a Low-carbohydrate Diet, Part II
I just found another very interesting study performed in Japan by Dr. Hajime Haimoto and colleagues (free full text). They took severe diabetics with an HbA1c of 10.9% and put them on a low-carbohydrate diet:
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
The main principle of the CRD [carbohydrate-restricted diet] was to eliminate carbohydrate-rich food twice a day at breakfast and dinner, or eliminate it three times a day at breakfast, lunch and dinner... There were no other restrictions. Patients on the CRD were permitted to eat as much protein and fat as they wanted, including saturated fat.What happened to their blood lipids after eating all that fat for 6 months, and increasing their saturated fat intake to that of the average American? LDL decreased and HDL increased, both statistically significant. Oops. But that's water under the bridge. What we really care about here is glucose control. The patients' HbA1c (glycated hemoglobin; a measure of average blood glucose over the past several weeks) declined from 10.9 to 7.4%.
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:One female patient had an increased physical activity level during the study period in spite of our instructions. However, her increase in physical activity was no more than one hour of walking per day, four days a week. She had implemented an 11% carbohydrate diet without any antidiabetic drug, and her HbA1c level decreased from 14.4% at baseline to 6.1% after 3 months and had been maintained at 5.5% after 6 months.That patient began with the highest HbA1c and ended with the lowest. Complete glucose control using only diet and exercise. It may not work for everyone, but it's effective in some cases. The study's conclusion:
...the 30%-carbohydrate diet over 6 months led to a remarkable reduction in HbA1c levels, even among outpatients with severe type 2 diabetes, without any insulin therapy, hospital care or increase in sulfonylureas. The effectiveness of the diet may be comparable to that of insulin therapy.
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
Diabetics on a Low-carbohydrate Diet, Part II
I just found another very interesting study performed in Japan by Dr. Hajime Haimoto and colleagues (free full text). They took severe diabetics with an HbA1c of 10.9% and put them on a low-carbohydrate diet:
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
The main principle of the CRD [carbohydrate-restricted diet] was to eliminate carbohydrate-rich food twice a day at breakfast and dinner, or eliminate it three times a day at breakfast, lunch and dinner... There were no other restrictions. Patients on the CRD were permitted to eat as much protein and fat as they wanted, including saturated fat.What happened to their blood lipids after eating all that fat for 6 months, and increasing their saturated fat intake to that of the average American? LDL decreased and HDL increased, both statistically significant. Oops. But that's water under the bridge. What we really care about here is glucose control. The patients' HbA1c (glycated hemoglobin; a measure of average blood glucose over the past several weeks) declined from 10.9 to 7.4%.
Here's a graph showing the improvement in HbA1c. Each line represents one individual:
Every single patient improved, except the "dropout" who stopped following the diet advice after 3 months (the one line that shoots back up at 6 months). And now, an inspirational anecdote from the paper:One female patient had an increased physical activity level during the study period in spite of our instructions. However, her increase in physical activity was no more than one hour of walking per day, four days a week. She had implemented an 11% carbohydrate diet without any antidiabetic drug, and her HbA1c level decreased from 14.4% at baseline to 6.1% after 3 months and had been maintained at 5.5% after 6 months.That patient began with the highest HbA1c and ended with the lowest. Complete glucose control using only diet and exercise. It may not work for everyone, but it's effective in some cases. The study's conclusion:
...the 30%-carbohydrate diet over 6 months led to a remarkable reduction in HbA1c levels, even among outpatients with severe type 2 diabetes, without any insulin therapy, hospital care or increase in sulfonylureas. The effectiveness of the diet may be comparable to that of insulin therapy.
Diabetics on a Low-carbohydrate Diet
The Tokelau Island Migrant Study: Diabetes
Heroin overdoses hit most CT towns, moving to suburbs and to older victims
A new study by researchers at the Yale School of Public Health finds that, on average, more than one CT resident died every other day from heroin overdose deaths in the last eleven years. That rate is rising; it may soon overtake automobile accidents as a cause of death. The problem is spreading out of cities into the suburbs; all but 22 of CT’s 169 cities and towns had a fatal overdose of either heroin or pharmaceutical narcotics between 1997 and 2007. At Blue Hills Substance Abuse Services in Hartford the proportion of young adults in treatment for heroin addiction has risen from 10 to 30 percent in recent years. Overdoses are rising among older victims becoming more common among middle aged residents than young adults because of changing physiology over the lifespan, according to the Yale Daily News. A series of articles in yesterday’s NY Times finds that CT is not alone – heroin use is up across the region. Experts blame heroin’s lower cost compared to other drugs and it is sold in more lethal forms now than in the 1970’s.
Ellen Andrews
Ellen Andrews
Sunday, September 27, 2009
No Need to Worry, No H1N1 virus could mutate
The researchers who made H1N1 vaccines could be relieved that the virus becomes a pandemic it could not prove the virus mutate into another type such as that previously had rumored.
Although the H1N1 virus has spread across nearly 50 countries around the world, but most cases are still in the mild or moderate degree, even almost the same as the common cold. But not a bit too must be treated in hospital.
The good news is that H1N1 viruses mentioned could mutate and turn into a new type of virus was not proven. Genetic test results prove that there is no any changes to the virus. Vaccine tested in October next plan was considered to be appropriate and may prevent the development of the virus.
"That means a vaccine that has been successful we will be very suitable production and there should be no more changes that can immediately stop its spread," said Dr. Thomas R. Frieden from the U.S. Centers for Disease Control and Prevention, as quoted by AP, on Monday (28/9/2009).
Frieden warned, before the vaccine was issued in October next, people are supposed to keep washing hands, covering mouth when you cough or sneeze and stay home if you feel sick.
Children and pregnant women are the group most at risk of H1N1 that are preferred in the provision of vaccines. Another group that should be prioritized are those who have heart disease, diabetes, respiratory problems and other medical personnel who deal with sick people.
To obtain the vaccine for children, the plan will be made vaccine clinic at each school. But even though health workers suggest the importance of vaccines for children, but according to a survey conducted CS Mott Children's Hospital National Poll on Children's Health of 1678 parents, only about 40 percent of it going to give vaccines to children.
As many as 46 percent of parents who are not too interested in providing vaccines for children say that they are not too worried that her son would be affected by H1N1 virus, while 20 percent believe that the virus is not too serious.
"It signifies the awareness of parents on the importance of H1N1 vaccine is still very low compared with the common cold. This perception must be changed because even if the H1N1 virus is not fierce as the H5N1 virus (bird flu) but still need to be anticipated," said Dr. Matthew Davis, a professor of Pediatrics and internal medicine in the Child Health Evaluation and Research Unit at the University of Michigan Medical School.
Previously, researchers in the United States also noted that the new H1N1 virus appears not competitive with seasonal flu, which can not mix with other flu viruses that circulate into
Although the H1N1 virus has spread across nearly 50 countries around the world, but most cases are still in the mild or moderate degree, even almost the same as the common cold. But not a bit too must be treated in hospital.
The good news is that H1N1 viruses mentioned could mutate and turn into a new type of virus was not proven. Genetic test results prove that there is no any changes to the virus. Vaccine tested in October next plan was considered to be appropriate and may prevent the development of the virus.
"That means a vaccine that has been successful we will be very suitable production and there should be no more changes that can immediately stop its spread," said Dr. Thomas R. Frieden from the U.S. Centers for Disease Control and Prevention, as quoted by AP, on Monday (28/9/2009).
Frieden warned, before the vaccine was issued in October next, people are supposed to keep washing hands, covering mouth when you cough or sneeze and stay home if you feel sick.
Children and pregnant women are the group most at risk of H1N1 that are preferred in the provision of vaccines. Another group that should be prioritized are those who have heart disease, diabetes, respiratory problems and other medical personnel who deal with sick people.
To obtain the vaccine for children, the plan will be made vaccine clinic at each school. But even though health workers suggest the importance of vaccines for children, but according to a survey conducted CS Mott Children's Hospital National Poll on Children's Health of 1678 parents, only about 40 percent of it going to give vaccines to children.
As many as 46 percent of parents who are not too interested in providing vaccines for children say that they are not too worried that her son would be affected by H1N1 virus, while 20 percent believe that the virus is not too serious.
"It signifies the awareness of parents on the importance of H1N1 vaccine is still very low compared with the common cold. This perception must be changed because even if the H1N1 virus is not fierce as the H5N1 virus (bird flu) but still need to be anticipated," said Dr. Matthew Davis, a professor of Pediatrics and internal medicine in the Child Health Evaluation and Research Unit at the University of Michigan Medical School.
Previously, researchers in the United States also noted that the new H1N1 virus appears not competitive with seasonal flu, which can not mix with other flu viruses that circulate into
src="http://pagead2.googlesyndication.com/pagead/show_ads.js" type="text/javascript">
Dallas Morning News' excellent series on health care costs (and other things that matter)
Hooray to the Dallas Morning News for its week-long series on health care and the systemic issues that have contributed to the crisis we are now in. Free registration may be required to view all of these articles. . . .Sun., 9/27: High prices, red tape fuel popular Dallas doctor's move to Temple Sun., 9/27: Focus on cost efficiency, quality pays off for Temple-based Scott & White Healthcare Sun.,
Vols-au-vent( Puff Pastry Shell)

The September 2009 Daring Bakers' challenge was hosted by Steph of A Whisk and a Spoon. She chose the French treat, Vols-au-Vent based on the Puff Pastry recipe by Michel Richard from the cookbook Baking With Julia by Dorie Greenspan.
Making the flaky,buttery puff pastry at home without anything artificial and at cheaper price ,was an incredible experience.Little time-consuming alright ,but if you can roll a dough then making the professional quality pastry dough is not impossible.The steps of making the supple ,smooth,lovely pastry dough are pretty straightforward,there is lot of waiting time and the dough has to be cold at all times,if possible also keep the rolling pin cold in the fridge.The filling variations are endless,fruity,savory or meaty,pick your choicest.So next time you are in the mood for the buttery goodness think of baking one of your own from the scratch.
Michel Richard’s Puff Pastry Dough
Puff pastry is in the ‘laminated dough” family, along with Danish dough and croissant dough. A laminated dough consists of a large block of butter (called the “beurrage”) that is enclosed in dough (called the “détrempe”). This dough/butter packet is called a “paton,” and is rolled and folded repeatedly (a process known as “turning”) to create the crisp, flaky, parallel layers you see when baked. Unlike Danish or croissant however, puff pastry dough contains no yeast in the détrempe, and relies solely aeration to achieve its high rise. The turning process creates hundreds of layers of butter and dough, with air trapped between each one. In the hot oven, water in the dough and the melting butter creates steam, which expands in the trapped air pockets, forcing the pastry to rise.
This wonderful on-line video from the PBS show “Baking with Julia” makes it easier to understand the procedure.
Prep Times:
-about 4-5 hours to prepare the puff pastry dough (much of this time is inactive, while you wait for the dough to chill between turns…it can be stretched out over an even longer period of time if that better suits your schedule)
-about 1.5 hours to shape, chill and bake the vols-au-vent after your puff pastry dough is complete
Recipe From: Baking with Julia by Dorie Greenspan
Yield: 2 pounds dough

Ingredients:
2 cups unbleached all-purpose flour
*1 cup cake flour
1 teaspoon white vinegar(optional)
1 teaspoon salt (you can cut this by half for a less salty dough or for sweet preparations)
1 cup (10 fl oz/ 300 ml) ice water
2 sticks cold butter very cold unsalted butter
plus extra flour for dusting work surface
*if you can't find cake flour use all purpose flour instead.
Method
Mixing the Dough:
Put the all-purpose flour, cake flour, and salt in a food processor and pulse a couple of times just to mix. Add the water all at once, pulsing until the dough forms a ball on the blade. The dough will be very moist and pliable and will hold together when squeezed between your fingers.
Remove the dough from the machine, form it into a ball, with a small sharp knife, slash the top in a tic-tac-toe pattern. Wrap the dough in a damp towel and refrigerate for about 5 minutes.
Meanwhile, place the butter between 2 sheets of plastic wrap and beat it with a rolling pin until it flattens into a square that's about 1" thick. Take care that the butter remains cool and firm: if it has softened or become oily, chill it before continuing.
Incorporating the Butter:
Unwrap the dough and place it on a work surface dusted with all-purpose flour (A cool piece of marble is the ideal surface for puff pastry) with your rolling pin, press on the dough to flatten it and then roll it into a square. Keep the top and bottom of the dough well floured to prevent sticking and lift the dough and move it around frequently. Starting from the center of the square, roll out over each corner to create a thick center pad with "ears," or flaps.
Place the cold butter in the middle of the dough and fold the ears over the butter, stretching them as needed so that they overlap slightly and encase the butter completely. (If you have to stretch the dough, stretch it from all over; don't just pull the ends) you should now have a package that is 8" square.
To make great puff pastry, it is important to keep the dough cold at all times. There are specified times for chilling the dough, but if your room is warm, or you work slowly, or you find that for no particular reason the butter starts to ooze out of the pastry, cover the dough with plastic wrap and refrigerate it . You can stop at any point in the process and continue at your convenience or when the dough is properly chilled.
Making the Turns:
Gently but firmly press the rolling pin against the top and bottom edges of the square (this will help keep it square). Then, keeping the work surface and the top of the dough well floured to prevent sticking, roll the dough into a rectangle that is three times as long as the square you started with.With this first roll, it is particularly important that the butter be rolled evenly along the length and width of the rectangle; check when you start rolling that the butter is moving along well, and roll a bit harder or more evenly, if necessary, to get a smooth, even dough-butter sandwich (use your arm-strength!).
With a pastry brush, brush off the excess flour from the top of the dough, and fold the rectangle up from the bottom and down from the top in thirds, like a business letter, brushing off the excess flour. You have completed one turn.
Rotate the dough so that the closed fold is to your left, like the spine of a book. Repeat the rolling and folding process, rolling the dough to a length of 24" and then folding it in thirds. This is the second turn.
Chilling the Dough:
If the dough is still cool and no butter is oozing out, you can give the dough another two turns now. If the condition of the dough is iffy, wrap it in plastic wrap and refrigerate it for at least 30 minutes. Each time you refrigerate the dough, mark the number of turns you've completed by indenting the dough with your fingertips. It is best to refrigerate the dough for 30 to 60 minutes between each set of two turns.
The total number of turns needed is six. If you prefer, you can give the dough just four turns now, chill it overnight, and do the last two turns the next day. Puff pastry is extremely flexible in this regard. However, no matter how you arrange your schedule, you should plan to chill the dough for at least an hour before cutting or shaping it.
Forming and Baking the Vols-au-Vent

Yield: 1/3 of the puff pastry recipe below will yield about 8-10 1.5” vols-au-vent or 4 4” vols-au-vent
Method
Line a baking sheet with parchment and set aside.
Using a knife or metal bench scraper, divided your chilled puff pastry dough into three equal pieces. Work with one piece of the dough, and leave the rest wrapped and chilled. (If you are looking to make more vols-au-vent than the yield stated above, you can roll and cut the remaining two pieces of dough as well…if not, then leave refrigerated for the time being or prepare it for longer-term freezer storage. See the “Tips” section below for more storage info.)
On a lightly floured surface, roll the piece of dough into a rectangle about 1/8 to 1/4-inch (3-6 mm) thick. Transfer it to the baking sheet and refrigerate for about 10 minutes before proceeding with the cutting.
Using a ¾-inch cutter for small vols-au-vent, or a 2- to 2.5-inch round cutter for large, cut centers from half of the rounds to make rings. These rings will become the sides of the vols-au-vent, while the solid disks will be the bottoms. You can either save the center cut-outs to bake off as little “caps” for you vols-au-vent, or put them in the scrap pile.
Dock the solid bottom rounds with a fork (prick them lightly, making sure not to go all the way through the pastry) and lightly brush them with water. Place the rings directly on top of the bottom rounds and very lightly press them to adhere. Brush the top rings lightly with water, trying not to drip any down the sides (which may inhibit rise).
Refrigerate the assembled vols-au-vent on the lined baking sheet while you pre-heat the oven to 400ºF (200ºC). (You could also cover and refrigerate them for a few hours at this point.)
Once the oven is heated, remove the sheet from the refrigerator . Bake the shells until they have risen and begin to brown, about 10-15 minutes depending on their size. Reduce the oven temperature to 350ºF (180ºC). If the centers have risen up inside the vols-au-vent, you can gently press them down. Continue baking until the layers are golden, about 15-20 minutes more. (If you are baking the center “caps” they will likely be finished well ahead of the shells, so keep an eye on them and remove them from the oven when browned.)
Remove to a rack to cool. Cool to room temperature for cold fillings or to warm for hot fillings.
Baked vols-au-vent shells can be stored airtight for a day.Shaped, unbaked vols-au-vent can be wrapped and frozen for up to a month
Vols-au-vent with Sweet Peach and Plum Filling
Prepare flavored sugar syrup by boiling 1/2 cup of water with 1/4 cup sugar with whole spices like cinnamon and cloves until thick and syrupy.Fish out the whole spices.
Thinly slice the ripe peaces and plums and arrange in baked shell( vols-au-vent).Pour about a tablespoon of syrup on each shell along the fruit filling.Bake on 350F for another 6-7 minutes and serve warm or cold.

The picture is my entry for Garnish the Dish over at Innovative In-laws(Nithya and Pavithra)
Saturday, September 26, 2009

Friday, September 25, 2009
Sleep, Drugs for Influenza
When exposed to cold, flu drugs are consumption and vitamin C is the first thing that occurred to someone. But you know, the most effective drugs to prevent and treat flu turned out to be sleeping enough.
A study has shown that those who sleep more easily with the flu, the researchers speculate that it is the accumulation of the lack of sleep. Insufficient sleep causes the body's immune system and the virus was less easy to enter.
In a study recently that found in the Archives of Internal Medicine, researchers conducted a study of 153 men and women for 2 weeks. Researchers checked the quality and quantity of respondents each day. Every 5 days, researchers in the room of respondents quarantine influenza virus.
Respondents who slept with a number of hours less than 7 or 8 hours a day were 3 times more frequent colds than those who slept an average of 8 hours a day.
Sleep and the immune system are closely linked. Less rest body will not have a good immune system because it was not given a chance to rest and produce defense cells that function against the virus.
Previous researchers also found that mammalian sleep was enough to produce levels of white blood cells that function to fight disease. White blood cells will increase, but not with red blood cells.
"The species with sufficient sleep duration would increase the immune system and body will be well protected," said researchers from the Max Planck Institute for Evolutionary Anthropology, was quoted as saying by the New York Times, Friday (25/9/2009).
Enough sleep was not only prevent someone from influenza disease, but also can treat it. If exposed to influenza, the system is disturbed metabolism, therefore the body needs to adapt again, and enough sleep can overcome this.
From now on, do not Sepelekan sleep problems and set your bedtime so your body always fit and able to work a maximum.
A study has shown that those who sleep more easily with the flu, the researchers speculate that it is the accumulation of the lack of sleep. Insufficient sleep causes the body's immune system and the virus was less easy to enter.
In a study recently that found in the Archives of Internal Medicine, researchers conducted a study of 153 men and women for 2 weeks. Researchers checked the quality and quantity of respondents each day. Every 5 days, researchers in the room of respondents quarantine influenza virus.
Respondents who slept with a number of hours less than 7 or 8 hours a day were 3 times more frequent colds than those who slept an average of 8 hours a day.
Sleep and the immune system are closely linked. Less rest body will not have a good immune system because it was not given a chance to rest and produce defense cells that function against the virus.
Previous researchers also found that mammalian sleep was enough to produce levels of white blood cells that function to fight disease. White blood cells will increase, but not with red blood cells.
"The species with sufficient sleep duration would increase the immune system and body will be well protected," said researchers from the Max Planck Institute for Evolutionary Anthropology, was quoted as saying by the New York Times, Friday (25/9/2009).
Enough sleep was not only prevent someone from influenza disease, but also can treat it. If exposed to influenza, the system is disturbed metabolism, therefore the body needs to adapt again, and enough sleep can overcome this.
From now on, do not Sepelekan sleep problems and set your bedtime so your body always fit and able to work a maximum.
src="http://pagead2.googlesyndication.com/pagead/show_ads.js" type="text/javascript">
Coverage of the BSA ruling in the blogosphere...
Not PC - BSA backs chiropractic quackery
DC's Improbable Science - Two lawyers and two journalists squash criticism of chiropractic on TV
MacDoctor - Broadcasting Substandards
Doctor.co.nz - Medical researcher gets it in neck
Tea, Blues, and Book Reviews - BSA vs Dr Shaun Holt: What can experts safely say?
BioBlog - a rather strange decision
Freedomain Radio - an FDR listener takes on chiropractors...
DC's Improbable Science - Two lawyers and two journalists squash criticism of chiropractic on TV
MacDoctor - Broadcasting Substandards
Doctor.co.nz - Medical researcher gets it in neck
Tea, Blues, and Book Reviews - BSA vs Dr Shaun Holt: What can experts safely say?
BioBlog - a rather strange decision
Freedomain Radio - an FDR listener takes on chiropractors...
Annual comparison of health plans out
The CT Insurance Dept. has released their 2009 Consumer Report Card on Health Insurance Carriers in CT. The report compares insurance plans on the number of participating providers and 14 quality measures including rates of cancer screening, immunization rates and the percent of physicians who are board certified. For example, the percentage of patients who’ve been hospitalized with heart disease who are now managed for their cholesterol levels varies from a low of 55.6% (Oxford) to a high of 74.3% (HealthNet). Eye exams for people with diabetes vary from 56.2% (Oxford) to 75.2% (ConnectiCare). Beta blockers after heart attacks ranged from 38.6% (ConnectiCare) to 100% (Aetna). The report also includes insurers’ customer appeal numbers; rates of denials that were reversed on appeal range from 25.8% (HealthNet) to 57.2% (Anthem). Medical loss ratios varied from 81.5% (Oxford) to 85.8% (ConnectiCare). The report also includes information on member satisfaction, prescriptions, mental health and substance abuse services as well as a very helpful glossary of terms. The comparisons are based on 2008 data. The report also includes insurer’s customer service phone #s and government agencies to call for help.
Ellen Andrews
Ellen Andrews
laptops wanted for community workers in Zambia

I have just returned from a trip with the charity Village Water to Zambia.
I’ve seen the charity pics but actually being taken by a villager to be shown the scoop hole they use for their drinking water is a whole different experience.
Village Water works in western Zambia providing safe water and hygiene and sanitation education for rural villages.
Three amazing ladies run the Mongu office – Clare, Precious and Albertina. I’m in awe of their strength, energy, optimism and dedication. They often work for 6-7 days a week. They think nothing of working long days going out to remote villages miles from electricity, mobile phone coverage or even tarmac roads.
They work with the villagers cajoling and teaching them, so that the villagers really own the wells put in by Village Water – they make a financial contribution to the cost of the well, someone in the village is trained to make repairs, and a village water committee (5 men and 5 women) ensures that the villagers put a little aside each month so they have the money to repair the pump when they need it. They build latrines and install simple hand washing facilities. Construct high tables so that pots and pans can be kept out of the reach of animals.
Since Village Water worked with them, many of the villages have started growing additional vegetables for sale and for consumption. One village got so excited by the water pump project they’ve now built a village community school and persuaded the Zambian government to provide them with a teacher. Another village has started pressing the government to provide a rural health centre close to them. All the villages reported that diarrhoea and other water-borne diseases had been virtually eliminated. Women are clearly empowered by the whole process.
Village Water funds are naturally concentrated on the water, sanitation and hygiene program, but at the end I asked the ladies what they needed to make their work easier. They said more office furniture and two more laptops. They already have one.
So here’s my questions: does anyone have a laptop they could donate (not more than 3 years old) or would like to buy a new one for these amazing ladies? Can anyone help with shipping them out to Western Province, Zambia?
If a laptop is beyond your means, you can still donate to the work of this amazing charity http://www.villagewater.org/home.html
I’m attaching a pic so you can see the ladies who would use it – Albertina on the left of the pic and Precious on the right of the pic.
Thanks
Jane Thurnell-Read
Preventing AIDS Vaccine Found
Bangkok, society might be a little berlega heart, because researchers have discovered a vaccine that can prevent a person infected with HIV to 31.2 percent. However, this vaccine can only prevent people infected, but can not treat people who are already infected.
The success of AIDS vaccine researchers made was announced in Bangkok on September 24, 2009. The vaccine is derived from the 2 previous vaccine failure and can protect people from AIDS infection for 31.2 percent. Currently being debated how to conduct testing with a limited number of vaccines that are owned and looking for ways to make better vaccines until keberhasilnnya reach a maximum 100 percent.
"The results of this research is a very important step to developing AIDS vaccines and was the first time in the world we have found a vaccine that can prevent HIV infection," says Thai Health Minister Withaya Kaewparadai, as quoted by Reuters on Friday (25/9/2009 ).
This vaccine is a combination of the vaccine Sanofi-Pasteur's ALVAC Canary pox / HIV and HIV vaccine failed AIDSVAX made by the company in San Francisco called VaxGen and is now owned by a nonprofit organization Global Solutions for Infectious Diseases. This experiment the U.S. government sponsored and conducted by the Thai public health ministry. This vaccine can reduce the risk of infection to 31.2 percent at 16,402 volunteers for 3 years.
The AIDS virus has infected about 33 million people worldwide and has killed 25 million people identified in the year since the 1980s. This affects the immune cells called T-cells. This discovery has instilled new hope in the field of HIV vaccine research and promised that an HIV vaccine is safe and very effective will be available for the entire population of the world most in need.
To be able to make AIDS vaccines required in-depth analysis and Dr. Donald Francis of Global Solutions for Infectious Diseases, adding that the company has limited the amount of remaining vaccine to test and make more vaccine.
Successfully created a vaccine that could help prevent HIV infection but could not do anything to reduce the virus already in the person's body. In addition to immune system response can be generated to protect anyone. In this study the vaccine is formulated specifically to work against two subtypes of human immunodeficiency virus (HIV) clade E, which is circulating in Thailand and Southeast Asia and the clade B circulating in the United States and Europe. The volunteers receive injections six times for more than 6 months with four shots and two ALVAC injections AIDSVAX. ALVAX is genetically engineered canarypox virus that has been incorporated into synthetic versions of three HIV genes, while AIDSVAX made using two versions of one HIV gene, one of subtype B and one from subtype E.
The success of AIDS vaccine researchers made was announced in Bangkok on September 24, 2009. The vaccine is derived from the 2 previous vaccine failure and can protect people from AIDS infection for 31.2 percent. Currently being debated how to conduct testing with a limited number of vaccines that are owned and looking for ways to make better vaccines until keberhasilnnya reach a maximum 100 percent.
"The results of this research is a very important step to developing AIDS vaccines and was the first time in the world we have found a vaccine that can prevent HIV infection," says Thai Health Minister Withaya Kaewparadai, as quoted by Reuters on Friday (25/9/2009 ).
This vaccine is a combination of the vaccine Sanofi-Pasteur's ALVAC Canary pox / HIV and HIV vaccine failed AIDSVAX made by the company in San Francisco called VaxGen and is now owned by a nonprofit organization Global Solutions for Infectious Diseases. This experiment the U.S. government sponsored and conducted by the Thai public health ministry. This vaccine can reduce the risk of infection to 31.2 percent at 16,402 volunteers for 3 years.
The AIDS virus has infected about 33 million people worldwide and has killed 25 million people identified in the year since the 1980s. This affects the immune cells called T-cells. This discovery has instilled new hope in the field of HIV vaccine research and promised that an HIV vaccine is safe and very effective will be available for the entire population of the world most in need.
To be able to make AIDS vaccines required in-depth analysis and Dr. Donald Francis of Global Solutions for Infectious Diseases, adding that the company has limited the amount of remaining vaccine to test and make more vaccine.
Successfully created a vaccine that could help prevent HIV infection but could not do anything to reduce the virus already in the person's body. In addition to immune system response can be generated to protect anyone. In this study the vaccine is formulated specifically to work against two subtypes of human immunodeficiency virus (HIV) clade E, which is circulating in Thailand and Southeast Asia and the clade B circulating in the United States and Europe. The volunteers receive injections six times for more than 6 months with four shots and two ALVAC injections AIDSVAX. ALVAX is genetically engineered canarypox virus that has been incorporated into synthetic versions of three HIV genes, while AIDSVAX made using two versions of one HIV gene, one of subtype B and one from subtype E.
src="http://pagead2.googlesyndication.com/pagead/show_ads.js" type="text/javascript">
Thursday, September 24, 2009
Another Fatty Liver Reversal, Part II
A month ago, I wrote about a reader "Steve" who reversed his fatty liver using a change in diet. Non-alcoholic fatty liver disease (NAFLD) is a truly disturbing modern epidemic, rare a few decades ago and now affecting roughly a quarter of the adult population of modern industrialized nations. Researchers cause NAFLD readily in rodents by feeding them industrial vegetable oils or large amounts of sugar.
Steve recently e-mailed me to update me on his condition. He also passed along his liver test results, which I've graphed below. ALT is a liver enzyme that enters the bloodstream following liver damage such as hepatitis or NAFLD. It's below 50 units/L in a healthy person*. AST is another liver enzyme that's below 35 units/L in a healthy person*.
Steve began his new diet in November of 2008 and saw a remarkable and sustained improvement in his ALT and AST levels:
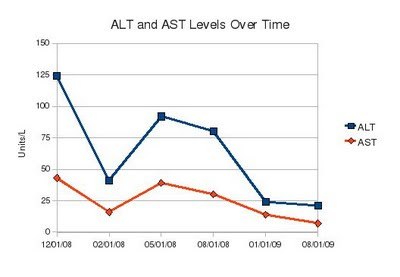 Here's how Steve described his diet change to me:
Here's how Steve described his diet change to me:
* The cutoff depends on who you ask, but these numbers are commonly used.
How to Fatten Your Liver
Excess Omega-6 Fat Damages Infants' Livers
Health is Multi-Factorial
Fatty Liver Reversal
Another Fatty Liver Reversal
Steve recently e-mailed me to update me on his condition. He also passed along his liver test results, which I've graphed below. ALT is a liver enzyme that enters the bloodstream following liver damage such as hepatitis or NAFLD. It's below 50 units/L in a healthy person*. AST is another liver enzyme that's below 35 units/L in a healthy person*.
Steve began his new diet in November of 2008 and saw a remarkable and sustained improvement in his ALT and AST levels:
 Here's how Steve described his diet change to me:
Here's how Steve described his diet change to me:I totally eliminated sugar, heavy starches, and grains. Started eating more whole, real foods, including things like grass-fed beef and pastured pork and eggs, began supplementing with good fats and omega-3 (pastured butter, coconut oil, cod liver oil). Ate more fruits and vegetables instead of refined carbs. Also completely gave up on the idea that I had to eat only "lean" meats. After my last results, the GI doc said that I wouldn't need the biopsy at all, that things were great, and that if I kept it up I "would live forever."He did experience some side effects from this diet though:
My triglycerides also went from pre-diet measures of 201 and 147 to post diet 86, 81, and 71.The liver is the body's "metabolic grand central station". It's essential for nutrient homeostasis, insulin sensitivity, detoxification, and hormone conversion, among other things. What's bad for the liver is bad for the rest of the body as well. Don't poison your liver with sugar and industrial vegetable oils.
The added bonus, of course, was that my weight went from 205 pounds to 162 pounds and my body fat percentage from 24% to 12% in the matter of five months--all without the typically excessive cardio I used to try unsuccessfully for weight loss.
* The cutoff depends on who you ask, but these numbers are commonly used.
How to Fatten Your Liver
Excess Omega-6 Fat Damages Infants' Livers
Health is Multi-Factorial
Fatty Liver Reversal
Another Fatty Liver Reversal
Subscribe to:
Posts (Atom)